

We are a tertiary referral center and often see patients from far and wide for second, third and seventh opinions! Complications of cosmetic surgical procedures of the face can be concerning to the surgeon as well as the patient. Most surgeons are skilled enough to correct any undesireable results. However, patients will often want second or third opinions. We also see many patients who want complications and undesireable results corrected.
IMPORTANT
not all unacceptable results are completely correctable. Certainly, when it comes to loss of tissue after repeated surgeries, an improvement can be sought, but a complete correction may not be possible
What complications of facial cosmetic surgery do you see?
The list of the types of patients we see is long. Some of the conditions we see are:

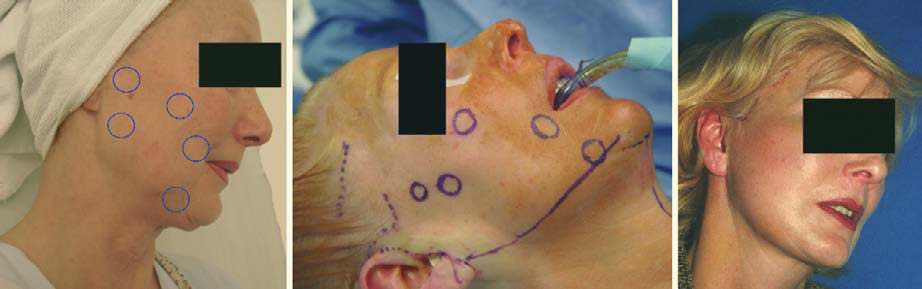
the wind-swept look where the incisions were not chosen wisely, the skin and sub-dermal changes were not properly assessed and the vectors for the lift chosen were for a “quick-lift” which was unwise.
Over-tight face after a facelift
We have all heard about the joker’s smile look and the over-tight face. Many of us have seen these results on the television screens and on the big screen. These are not easy problems to treat once the overly tight facelift or necklift has been performed. However with a careful review of the operation reports and examination of the patient, we can often improve the “pulled look” appearance.

Surgical correction of the wind-swept look and correction of the earlobe that is pulled downwards and forwards with loss of the earlobe is complex and much more difficult than doing the facelift and necklift properly in the first place. However, with a combination of revision surgery, scar replacement, fat grafts and lasers, a reasonably nice result can be obtained as seen here.
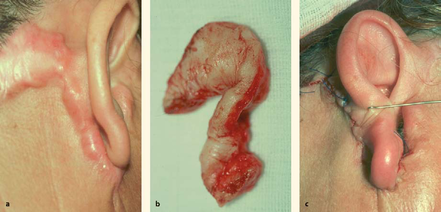
Earlobes pulled down and stuck to the face with loss of earlobes and with a wind-swept look
The earlobes pulled down and stuck to the face after a facelift and necklift.
This is a common problem that we see. It is possible to revise the scars and improve the position of the ear lobe and, in some cases, to even make a new “hanging” earlobe so that the face looks natural.
"I call it my botched facelift: I went to see Dr. Patel but his waiting list was longer than I was willing to wait. I made the mistake I dread every day of going to the next surgeon and having surgery done the following week! I was left with a too-tight pull, I got funny lines I never had, and worse of all, pain in my neck. I finally ." D. Rock 63 Yrs Old with Fat Droopy Eyes - Salt Lake City, UT
Pull lines on the face after a facelift

Bad scars, loss of earlobe and pull lines which make the jawline and neck look less than ideal
Pull lines on the face after a facelift: many patients succumb to the temptation of “weekend facelifts”, quick facelifts, etc. These are done through small incisions which can result in abnormal tension on the facial skin, resulting in “pull lines” which we also call kite lines. In such cases, it is necessary to redo the facelift and neck lift and change the vectors of the tissue repositioning, often with the use of other modalities like fat grafts, lasers, etc. We can improve these pulled faces.
Inadequate improvement of the jowls, jawline and neck after a facelift


Inadequate correction after a facelift and necklift with unacceptable scars. Correction was obtained by re-doing this patient’s facelift and necklift, fat grafts were used to correct the indentations, scar revision and repositioning was performed.
Facelift and necklift surgery are precise surgical techniques that depend upon experience, a detailed knowledge of anatomy and a careful study of aging of men and women. A careful preoperative analysis and planning are vital. If and when
Quick and template-type facelifts and necklifts are performed, the improvement can be moderate and unsatisfactory. About 30% of our facelifts are revision facelifts performed for patients who are either dissatisfied with their results from surgery elsewhere or where the results have not lasted sufficiently long enough after surgery.
Before & after

Revision facelift where tissue repositioning had been obtained but attention had not been paid to soft tissue volume loss and ptosis.

Therefore, the paient was left with residual facial and neck laxity and volume loss. A revision facelift and necklift with fat grafts, tissue repositioning, scar revision, correction of the chin and platysmal bands yielded a beautiful result.

This patient came to see us with an unacceptable result from a facelift and necklift. The choice of incisions was wrong, the pull was only vertical, resulting in “kite lines” or “wind-swept” lines, and the changes affecting the skin and dermal tissues was ignored, exacerbating the “surgical pulled look”
Treatment of skin changes: pores, vessels, pigment spots, wrinkles, lines, scars, etc
Some surgeons will perform very nice facelifts and necklifts but ignore the canvas of the face: the skin. A beautiful face demands beautiful skin as well as excellent underlying anatomical structures. We often see patients where the skin has been neglected: here we can achieve a lot of improvement using a combination of lasers, peels, pulsed light lasers, radiofrequency lasers, injection radiofrequency and other non-surgical techniques.
Before & After

with proper assessment and treatment, the skin can be improved together with deeper tissues
"I had a excellent eye lift done by Dr. Patel. He knows what he is doing and is very pleasant. Dr.Patel was easy to get an appointment and he works with you. The office staff was very pleasant and made you feel calm." D. Gull Highly recommended for eye lift surgery - Salt Lake City, UT
Badly placed scars after a facelift and necklift
The designing of the incisions is a very precise technique and is not the same in men and in women and, indeed, is not same from one face to another. We often see scars that are obvious and very anterior to the ear or hairline. In others, the scars are too wide and distort the ear or the face. In such cases, we carry out scar revisions of various kinds to improve and hide as much as possible the old scars and reduce the size and improve the location.
Asymmetry after Facelifts and Necklifts
We sometimes see patients who have a different result between the right and left sides of the face after a facelift and necklift. There are many reasons for this outcome, including underlying anatomical and bony differences between the two sides, different tissue placements, different incision placements, inadequate tissue volume replacement (fat grafts) and facial nerve and muscle problems. In some cases these can be improved, but one needs to see and examine the patients to obtain a detailed understanding of the underlying causes.







Facial Scars
We often see patients with unacceptable scars from trauma, surgery, tumour resection, reconstructive surgery, and other reasons. Depending upon the age, site, depth and relative relations, proper scar revision is planned using a combination of techniques, including lases, Z-plasty, W-plasty, geometric broken line scar revision, fat grafts, dermabrasion, microneedling, radiofrequency, vascular lasers and collagen remodeling lasers, among other techniques.

Scar revision with multiple Z-plasties
Keloid scar after a facelift revised with appropriate resection, repair and use of anti-scarring injections

Reconstructive surgery is more difficult than cosmetic surgery as it demands creation of tissues that are lost to trauma and scars which are associated with irregular scars and tissue loss. With appropriate planning, repair and recreation of anatomical planes, good outcomes can be obtained. The same principles apply to complications of cosmetic surgery.
Asymmetric eyelids and brows
After endoscopic browlift surgery and upper blepharoplasty, some degree of asymmetry is to be expected as none of us have the two sides look exactly the same. However, if the difference is very noticeable, it can be a problem. There are many reasons for this to occur, including failure to position the brows properly, failure to correct underlying ptosis of the eyelids, failure to design skin creases that match, failure to address the fatty tissue of the upper eyelid fat pads, too much removal of fat from eyelids and brows and misplacement of eyelid incisions, among other causes! As we talk to one another by looking at our eyes, designing eyelid surgery has to be the most fussy and accurate
of all plastic surgery procedures.

overly operated upper blepharoplasty with excessive removal of skin and fat and over-tightening of the levator tendons resulting in an inability to close the eyelids.

Poorly planned upper lid surgery with right retraction of the upper lid and asymmetrically performed removal of tissues.

Correction of the asymmetry of the upper and lower eyelids with reconstructive surgery
Unable to close eyelids after upper and/or lower eyelid surgery
This is a very common problem we see when the surgeon may have been over-zealous with the resection of tissues, or, not infrequently, the patient has asked the surgeon “to remove as much as he or she can” during the surgery, which is always a mistake. Again, proper planning with an assessment of the position of the eyeballs (proptosis, enophthalmos, etc), corneal health, laxity of tendons, looseness of eyelid tissues, ptosis or retraction, canthal dystopia, muscle tone, skin condition, degree of sun damage, etc, etc, etc are all factors that careful surgeons take into account. If you come to see us with the inability to close your eyelids after surgery, it is important for you to come with your preoperative photographs, and all your operation reports and clinical notes so we can examine you and assess your condition as well as what was done. Correction of this problem may involve one of myriad techniques and it may not
be possible to completely correct the problems.



Lower eyelids pulled down and away from the eyeball after lower blepharoplasty
Again, this is a not uncommon problem we see. In some instances, we can correct this with a minor procedure and some conservative treatment. In other cases, a more detailed procedure or procedures may be necessary.

Correction of lower eyelid malposition after cosmetic lower blepharoplasty
Abnormal incisions and scars after blepharoplasty and asymmetric results
Designing skin creases and placement of incisions when performing upper and lower blepharoplasty is the secret to hiding the incisions. No surgeon can create invisible incisions but with proper design, we can hide them well enough to not be noticeable by anyone except by the patient and by us! When the scars are not well places, revision may be possible but not with perfect results in every case. Again, it is important for you to bring your pre-surgical photographs and operation and clinical notes with you.

severe chemosis after lower blepharoplasty caused by injury to the nerves and muscles of the lower eyelid. Treatment needs to be urgent and due attention needs to be paid to protecting the cornea

Fat removal left this patient with loose skin (festoons). Correction involves attention to skin and deeper tissues.
Misplaced implants in the face

Misplaced implants in the face can be cheek, chin or other implants. Implants on the face should be inserted conservatively and with the smallest size possible to give a nice result, so as to avoid the “operated look.” Sterility is also vital to avoid the risk of infection of the face and the implanted areas. Here, we often need to completely remove the implants, allow the tissues to recover from the surgical trauma and then carry out further reconstruction, often with tissue repositioning and with fat grafts. Replacement implants are only used occasionally in such cases.
Facial plastic surgery gone bad

BEFORE & AFTER

After we performed corrective brow, eyelid and facial surgery to return him to his normal handsome face